Cervical (Cervix) Cancer: Types, Symptoms, Diagnosis, Treatment - PMCC Denver Oncology

Cervical cancer is the most frequent and deadly neoplastic disease in the female population, being the first cause of death due to malignant neoplasms in women aged 25 to 64 years. It is important to mention that in recent years the incidence of this type of cancer has increased in women under 50 years of age. Each year about 500,000 new cases are diagnosed worldwide. It is estimated that it produces around 231,000 deaths per year, 80% of which occurs in developing countries.
High-risk areas include South America, East and South Africa and India. In the United States there are more than 10,000 new cases per year with more than 3,700 deaths per year attributed to this disease. Survival of this disease is strongly influenced by the socioeconomic factor, which reflects the importance of access to organized programs for early detection and treatment.
Cervix Cancer Risk Factors
Women from 25 to 64 years of age
Start of sexual relations before the age of 18
History of sexually transmitted diseases
Cervicovaginal infection by the human papillomavirus (HPV)
Multiple sexual partners
Smoking
Denutrition
Deficiency of antioxidants
Immunodeficiency
Etiopathogenesis (Causes)

image source: kidshealth.org.nz
The normal cervix is composed of different types of epithelial cells; the middle cervical canal and the superior cervix are composed of secretory columnar epithelium (small neoplastic potential). The vagina, the ectocervix, and the distal cervical canal are composed of squamous epithelium (small neoplastic potential).
The squamocolumnar junction is the point where the squamous and columnar cells meet. This union is typically found between the ectocervix and the lower cervical canal, but the location varies throughout a woman's life. The original squamocolumnar junction is a transformation zone in which the change from one mature cell type to another (metaplasia) occurs. The metaplasia zones have high neoplastic potential.
In women of reproductive age, the squamocolumnar junction moves outward due to hormonal influence. The acidic vaginal pH causes mechanical irritation that induces the process of squamous metaplasia, resulting in a new squamocolumnar junction. This area between the original and the new squamocolumnar junction is referred to as the transition zone. Immature metaplastic squamous cells in this transformation zone are the most vulnerable to neoplasia.
The majority of squamous cell carcinomas originate in the squamocolumnar junction. In young women, the squamocolumnar junction is located outside the external cervical os and the tumor tends to grow outward (exophytic growth), in contrast, in older patients, the squamocolumnar junction is located in the cervical canal, so that cancer tends to grow inward (endophytic growth). HPV infection is associated with a high degree of cervical lesions and is considered the causative agent in the development of cervical cancer.
Get Full Guidance with Cancer & Disease Prevention, Screening, & Treatment

Human Papillomavirus (HPV)

image source: ucsfhealth.org
HPV infection is extremely common, these infections are typically associated with low-grade dysplastic lesions, which usually do not go beyond. However, persistent HPV infection is associated with high-grade dysplastic lesions that lead to the development of cervical cancer. It has been shown that 87% of squamous cell carcinomas and 77% of cervical adenocarcinomas are associated with HPV infection.
The persistent infection is due to a complex interaction between biological and immunological factors of the individual. Epidemiological studies suggest that infection with herpes simplex virus type II, the use of oral contraceptives for a long time, smoking and multiparity increase the risk of persistent HPV infection.
In the vast majority of women, the period between HPV infection and the development of dysplasia and/or invasive carcinoma is from years to decades, which offers great potential for early detection and early treatment to change the natural course of the disease and the morbidity associated with this disease.
The serotypes of HPV have been divided by molecular studies in groups of high, intermediate and low risk for the development of cervical neoplasia. Low-risk subtypes are associated with condylomata acuminata, intermediate and high-risk subtypes are associated with cervical dysplasia and invasive carcinoma. The serotypes most associated with the development of cancer are HPV-16 and HPV-18. The identification of high-risk serotypes has been important to define the therapeutic target in the prevention of cervical carcinoma.
Recently, a vaccine was developed to prevent HPV infection against high-risk subtypes that induce an immune response before HPV infection. It is ideal to administer it before the infection; however, it can also be given to people who have contracted the infection, since this prevents infection by other subtypes. The vaccine is approved by the FDA for administration in women between nine and 26 years of age.
Histological Types of Cervix Cancer
The World Health Organization (WHO) recognizes two main histological types of invasive cancer: squamous cell carcinoma, which constitutes about 75% of all cases of cervical cancer and adenocarcinoma that constitutes about 15-25% of cases. Other types of carcinoma such as adenosquamous carcinoma, cystic adenoid carcinoma, and metastatic carcinoma constitute the remaining 3-5% of cases.
Clinical Manifestations
Early stage cancer is usually asymptomatic, therefore screening with cytological evaluation of the endocervix and exocervix is necessary. Some symptoms that may occur are postcoital discomfort, intermenstrual or postmenopausal bleeding, vaginal discharge, weight loss, and pelvic pain due to uterine contractions caused by the accumulation of menstrual blood in patients with endocervical canal occlusion.
Mild chronic bleeding can cause anemia in some patients. Heavy bleeding is rare, but it can occur in advanced stages. In advanced cases, pelvic pain and lower extremity edema may occur due to occlusion of lymphatics or venous thrombosis of the external iliac vein.
Cervix Cancer Diagnosis
The presumptive diagnosis of cervical cancer can be established by clinical examination, cervical cytology (pap smear) or colposcopy. The definitive diagnosis is established only with histopathological examination by means of a colposcopy-directed biopsy.
PAP Test
The Papanicolaou test is a procedure used to obtain cervical cells in order to observe them under a microscope and detect if there is cancer or a premalignant lesion.
To take the sample, the doctor first places a speculum inside the patient's vagina. This metal or plastic instrument keeps the vagina open, so the doctor can properly evaluate the cervix. Then a sample of cells and mucus from the ectocervix is obtained by light scraping with a small spatula. A small brush or cotton swab is then inserted into the opening of the cervix to take a sample from the endocervix.
Although the Papanicolaou test has been more successful than any other cancer screening test, it is not infallible. One of the limitations of the Papanicolaou test is that the results need to be examined by the human eye, so accurate analysis of hundreds of thousands of cells in each sample is not always possible.
Colposcopy
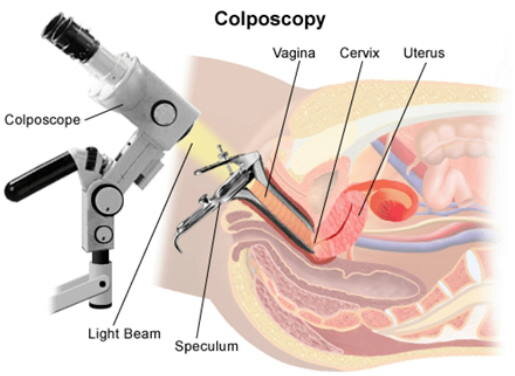
image source: obgynfl.com
If you have certain symptoms that suggest cancer or if the Pap test result shows abnormal cells, a colposcopy will be necessary.
During the test, a speculum is placed in the vagina to help the doctor look at the cervix. The doctor will use the colposcope to examine the cervix. This instrument remains outside the body and has magnifying lenses that allow the doctor to see up close and clearly the surface of the cervix. Usually, the doctor applies a dilute solution of acetic acid to the cervix to highlight any abnormal areas. If an alteration is observed, the doctor should perform a biopsy.
Have A Question About Cervix Cancer Screening, Prevention or Treatment?
Contact Our Office.
Call 720.893.9515
Cervical Biopsies
Several methods can be used to obtain the sample needed to perform the histological study. If the biopsy can completely remove all abnormal tissue, this may be the only treatment needed.
Colposcopic Biopsy
For this type of biopsy, the cervix is first examined with a colposcope to detect abnormal areas, if there is an injury, biopsy forceps are used to remove a small section (approximately 1/8 inch) from the affected area.
Endocervical Curettage (Endocervical Scraping)
On some occasions, the transformation zone cannot be evaluated with the colposcope, and an additional procedure has to be done to examine that area and determine if there is cancer. This involves scraping the endocervix by inserting a curette into the endocervical canal and removing some tissue that is then sent to the laboratory for histological examination.
Cone Biopsy
In this procedure, also known as conization, a cone-shaped piece of tissue is removed from the cervix. The base of the cone is constituted by the exocervix, and the tip or apex of the cone is formed by the endocervical canal. The tissue that is removed in the cone includes the transformation zone. A cone biopsy can also be used as a treatment to completely remove many pre-cancers, as well as cancerous tumors at very early stages.
Computed Tomography
Computed tomography (CT) is the most widely used method to rule out the local or distant spread of cancer.
Cervix Cancer Treatment
Cervix Cancer Surgery
Depending on the stage of the disease and the extent of the tumor, the surgeon will decide the amount of tissue to be removed. The main types of surgery performed are:
Conization: consists of the exeresis of a fragment of cone-shaped tissue that includes the exocervix and the transformation zone.
Radical trachelectomy: This surgery is used to remove the cervix and pelvic lymph nodes, leaving the uterus intact.
Hysterectomy: Simple hysterectomy involves the removal of the uterus and cervix, while radical hysterectomy involves the removal of the uterus and cervix, the upper third of the vagina, and the pelvic lymph nodes.
Pelvic exenteration: It is done in those cases in which the cancer has spread to neighboring organs. The uterus, vagina, lower colon, rectum and / or bladder are removed.
Radiotherapy

image source: medicalnewstoday.com
It consists of the application of high energy x-rays or radioactive particles to destroy cancer cells. It can be used as a single treatment before surgery or in combination with chemotherapy.
Chemotherapy
It is usually administered to eliminate malignant cells that may remain after surgery or radiation therapy. The most commonly used medications to treat cervical cancer include: Cisplatin, Carboplatin, Paclitaxel, Topotecan, Gemcitabin.
Explore Cancer & Disease Prevention, Screening, & Treatment
Have A Question About Cervix Cancer Screening, Prevention or Treatment?
Contact Our Office.
Call 720.893.9515
Sources
1. Smith R, Cokkinides V, Brawley O. Cancer screening in the United States, 2009: a review of current American Cancer Society guidelines and issues in cancer screening. CA Cancer J Clin 2009; 59: 27-41.
2. Jhingran A. Abeloff: Abeloff’s Clinical Oncology. 4th. Ed. Chap. 91. Cancers of the cervix, vulva, and vagina; 2008
3. Kahn J. HPV Vaccination for the Prevention of Cervical Intraepithelial Neoplasia. NEJM 2009; 361(3): 271-8.
4. Marth, C. et al. Cervical cancer: ESMO Clinical Practice Guidelines for diagnosis, treatment and follow-up. Ann. Oncol. 28, iv72–iv83 (2017).