Gastric (Stomach) Cancer: Types, Symptoms, Diagnosis, Treatment - PMCC Denver Oncology

Gastric adenocarcinoma or more commonly referred to as Gastric cancer (cancer of the stomach) is a type of cancer that forms in the tissues that line the stomach. The lesion usually starts in the cells of the inner layer of the stomach (the mucosa), which is responsible for making and secreting mucus, gastric acid (HCL) and other substances.
Stomach cancer is the third most frequent tumor and the second cause of death related to cancer in the world. Despite this, its incidence and mortality have decreased in the last fifty years, especially in developed countries. This decrease can be explained by the improvement of the socioeconomic conditions that result in better nutritional education, increased consumption of fresh fruits, vitamins and vegetables, and better food preservation.
The increase in survival has been greater in Japan, a country where screening programs have detected up to 40% of tumors in early stages (in Europe they represent less than 15%). Stomach cancer shows a clear geographical variation (its incidence is higher in Chile, Colombia, Peru, South Korea, Japan and other Eastern countries), usually affects elderly people (80% of cases diagnosed correspond to people older than 65), it is more common in men (almost double than in women) and is associated, consistently, with a poor economic status.
Gastric Cancer Etiology

image source: heartburntucson.com
The development of gastric cancer is primarily due to the interaction of dietary, environmental and genetic factors.
Dietary and Environmental Factors
There is a great relationship between the incidence of gastric cancer and a diet with high salt intake and poor in fresh fruits and vegetables, low intake of vitamins A, C and E and micronutrients (selenium), as well as the consumption of food with methods of preservation with possible carcinogenic effect, such as smoked, salted and pickled.
Gastric cancer has also been linked to the concentration of nitrites in the diet and in drinking water. The bacteria present in the mouth and stomach would reduce the nitrites to nitrates that could lead to the formation of nitrosamides and nitrosamines, which have a known mutagenic and oncogenic effect. Gastric hypoacidity, vitamin C and E deficiency and bacterial contamination of food favor this process.
It has been shown that H. pylori infection is carcinogenic to humans, accounting for about 40% of all gastric cancers. Its prevalence in the general population is very high, although it seems that some strains, such as cagA, are more involved in carcinogenic processes.
Other environmental factors such as alcohol and tobacco consumption are also related to the development of gastric cancer. The occurrence of stomach adenocarcinoma after prolonged administration of antisecretory medication such as H2-antagonists or proton pump inhibitors has also not been demonstrated.
Get Full Guidance with Cancer & Disease Prevention, Screening, & Treatment

Stomach Cancer Genetic Causes
Individuals with a first degree relative affected by stomach cancer have two to three times more risk of developing this neoplasm. The most common genetic alterations related to gastric adenocarcinoma are: the presence of mutations in the TP53, APC genes (in the context of familial adenomatous polyposis) and E-cadherin.
Types of Gastric Adenocarcinoma
Adenocarcinoma is the most common tumor of the stomach (90%). There are two histological subtypes of gastric adenocarcinoma, intestinal and diffuse, with epidemiological and prognostic differences. The intestinal type is characterized by the formation of tubular structures similar to the intestinal glands, it usually affects the distal part of the stomach and is more frequent in elderly people.
This type of cancer develops from chronic atrophic gastritis, induced by environmental and dietary risk factors. This form of neoplasia tends to occur in regions with a high incidence of gastric cancer and represents the form of cancer that is experiencing a global decrease.
On the other hand, diffuse gastric adenocarcinoma does not present any glandular structure. It is more common in young people and in people of blood group A, is not usually associated with precancerous lesions and is more related to hereditary factors. Their frequency is similar anywhere in the world and they have a worse prognosis than the intestinal form.
Clinical Manifestations
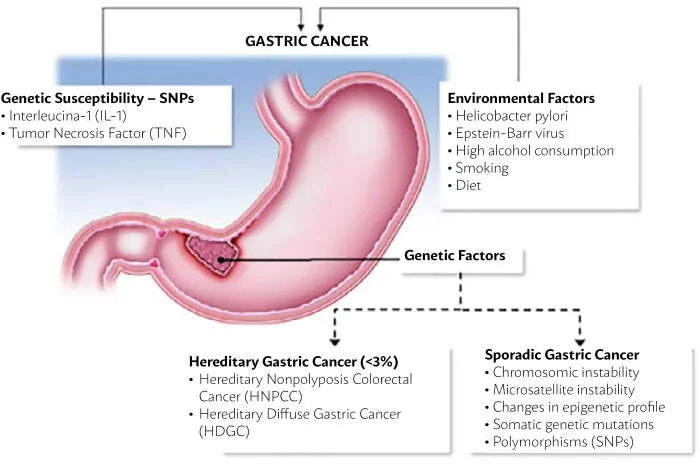
image source: scielo.br
Gastric cancer, when superficial and potentially curable, usually does not produce symptoms. Therefore, the disease is usually locally advanced when the diagnosis is suggested by the presence of clinical manifestations. The main symptoms associated with gastric cancer are difficulty swallowing, weight loss, anemia, anorexia, dyspepsia, palpable abdominal mass, abdominal pain, nausea, vomiting, among others.
Some of the symptoms mentioned suggest a certain location. This is the case of the difficulty swallowing in tumors that infiltrate the cardia or the presence of nausea and vomiting when the tumor causes partial or total obstruction of the pylorus. The physical examination is usually normal. When the diagnosis is made, there is usually metastasis, which frequently affects the liver (40%), lung, peritoneum and bone marrow.
It is important to highlight the efficacy of proton pump inhibitors to heal malignant ulcers, so it is advisable to establish a diagnosis before these agents are used to treat patients with risk factors.
Gastric Cancer Diagnosis
The diagnostic technique of choice for suspected gastric cancer is upper digestive endoscopy, which allows establishing the exact location of the lesion and taking biopsies for histological study. The double contrast radiological study may suggest the presence of a neoplasm when an asymmetric ulcer bed, mass or loss of gastric compliance is observed.
Laboratory studies are usually normal until the cancer is advanced. The occurrence of anemia (42% of patients) indicates chronic bleeding from the lesion. The elevation of liver enzymes (26%) may reflect the tumor invasion of the liver. Unfortunately, there are currently no specific serum tumor markers for this type of tumor. However, although the monitoring of carcinoembryonic antigen levels is not useful for the early diagnosis of these patients, it can be useful in its postoperative follow-up.
Extension Diagnosis
The completeness of the tumor staging will depend both on the patient's clinical situation and on the therapeutic possibilities. Computed tomography (CT) is useful for the detection of distant metastases and for the evaluation of regional lymph nodes.
Endoscopic ultrasonography (EUS) is superior to CT for the local staging of gastric cancer, since it allows visualizing the layers that make up the gastric wall, which makes it the best imaging study to determine the depth of tumor invasion. In addition, its capacity for the detection of perigastric nodes is comparable to that of CT. Another advantage of this technique is that it allows fine needle aspiration with which cytological confirmation of metastatic adenopathies can be obtained.
Laparoscopy allows establishing the resectability of the tumor with a diagnostic accuracy of more than 90%, which avoids up to 40% of unnecessary laparotomies. The washing of the peritoneal cavity allows detecting the presence of tumor cells in the peritoneum, which also has prognostic value.
Have A Question About Gastric Cancer Screening, Prevention or Treatment?
Contact Our Office.
Call 720.893.9515
Gastric Cancer Treatment
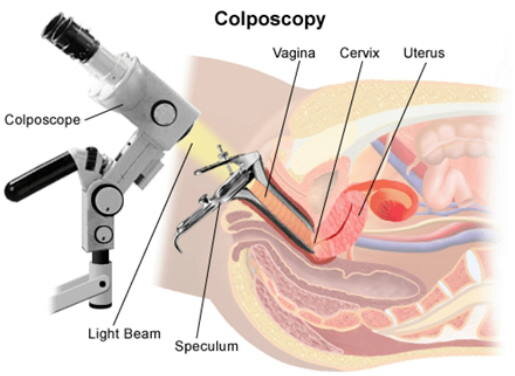
image source: obgynfl.com
Cervix Cancer Surgery
Depending on the stage of the disease and the extent of the tumor, the surgeon will decide the amount of tissue to be removed. The main types of surgery performed are:
Conization: consists of the exeresis of a fragment of cone-shaped tissue that includes the exocervix and the transformation zone.
Radical trachelectomy: This surgery is used to remove the cervix and pelvic lymph nodes, leaving the uterus intact.
Hysterectomy: Simple hysterectomy involves the removal of the uterus and cervix, while radical hysterectomy involves the removal of the uterus and cervix, the upper third of the vagina, and the pelvic lymph nodes.
Pelvic exenteration: It is done in those cases in which the cancer has spread to neighboring organs. The uterus, vagina, lower colon, rectum and / or bladder are removed.
Radiotherapy

image source: medicalnewstoday.com
It consists of the application of high energy x-rays or radioactive particles to destroy cancer cells. It can be used as a single treatment before surgery or in combination with chemotherapy.
Chemotherapy
It is usually administered to eliminate malignant cells that may remain after surgery or radiation therapy. The most commonly used medications to treat cervical cancer include: Cisplatin, Carboplatin, Paclitaxel, Topotecan, Gemcitabin.
Explore Cancer & Disease Prevention, Screening, & Treatment
Have A Question About Cervix Cancer Screening, Prevention or Treatment?
Contact Our Office.
Call 720.893.9515
Sources
1. Smith R, Cokkinides V, Brawley O. Cancer screening in the United States, 2009: a review of current American Cancer Society guidelines and issues in cancer screening. CA Cancer J Clin 2009; 59: 27-41.
2. Jhingran A. Abeloff: Abeloff’s Clinical Oncology. 4th. Ed. Chap. 91. Cancers of the cervix, vulva, and vagina; 2008
3. Kahn J. HPV Vaccination for the Prevention of Cervical Intraepithelial Neoplasia. NEJM 2009; 361(3): 271-8.
4. Marth, C. et al. Cervical cancer: ESMO Clinical Practice Guidelines for diagnosis, treatment and follow-up. Ann. Oncol. 28, iv72–iv83 (2017).