Thyroid Cancer: Types, Symptoms, Diagnosis, Treatment - PMCC Denver Oncology
Thyroid Cancer represents approximately 3% of all malignant tumors, and is the most common endocrine neoplasm, ranking fifth in frequency in women in the USA. It is more frequent in women than in men, in a 3: 1 ratio.
Thyroid cancer has an approximate incidence of 9 cases per 100 000 inhabitants, the maximum incidence is observed in women at 40 years and in men at 60 years. In most patients the etiology is unknown, but according to studies, radiation is an important factor.
Thyroid cancer is slow growing and usually responds well to treatment and can often be cured with radioactive iodine (when indicated). Even though thyroid cancer is advanced, there is an effective treatment for the most common forms of this cancer.
Thyroid Cancer Etiology
The process of oncogenesis (formation of cancer) is due to the interaction between genetic and environmental factors that alter the control of cell proliferation and differentiation. It is important to consider that ionizing radiation is the only etiological factor solidly related to the development of thyroid cancer.
Radiation: Several studies have shown that exposure to high doses of radiation, mainly during childhood, greatly increases the risk of developing thyroid cancer. This is often observed in cases where radiation is used to treat conditions such as acne, thymus enlargement, lymphomas, leukemia, etc. In most cases, thyroid cancer appears 20-40 years after exposure to radiation. These tumors are usually multifocal, but with a slow and favorable evolution.
Genetic Factors: They are observed mainly in the medullary carcinomas, which can develop in an isolated way in a 75% or associated to the MEN2 syndrome in 25% of the cases, these are inherited in an autosomal dominant way, mainly with the germinal mutation in the RET protooncogen.
Types of Thyroid Cancer
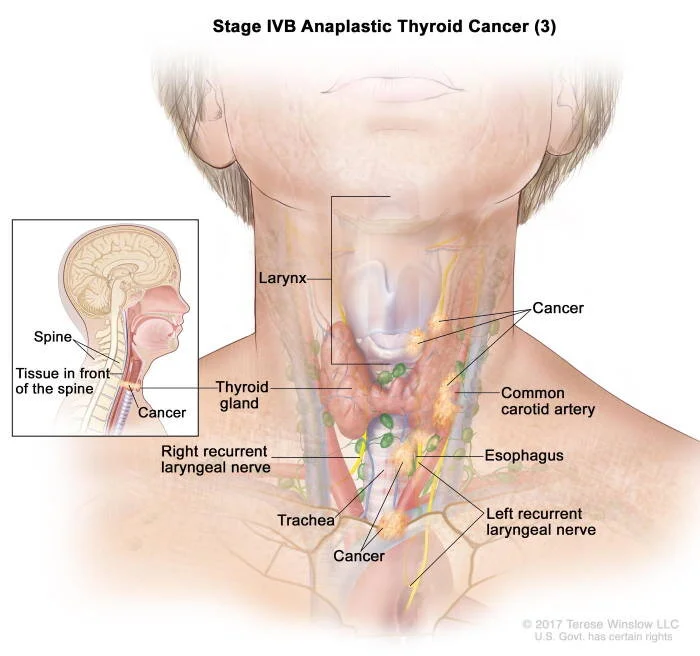
image source: cancer.gov, Terose Winslow LLC
Thyroid Papillary Cancer:
It is the most common, represents 80-85% of thyroid cancer, has a good prognosis and tends to spread through the lymphatic system; rarely presents distant metastasis, but in cases of presentation, the most affected organs are lung and bone.
Follicular Cancer:
It is the second in incidence and represents 15% of thyroid cancer, tends to spread by hematogenous, resulting in bone, lung and brain metastases. Metastases to lymph nodes are rare.
Papillary and follicular cancers are also known as Well-Differentiated Thyroid Cancer.
Anaplastic Cancer:
It occurs in 1-2% of patients, are aggressive invade nearby tissues quickly, occurs mainly in women over 60 years; They are unfavorable and most patients die approximately 6 months after diagnosis.
Medullary Cancer:
It represents 5-10% of the cases, it originates from the C cells of the thyroid, which produce calcitonin, the mutations of the proto-oncogene RET in the germinal line that can be seen in the MEN2 syndrome are characteristic. These tumors usually secrete calcitonin and carcinoembryonic antigen that can be used as tumor markers.
Get Full Guidance with Cancer & Disease Prevention, Screening, & Treatment

Thyroid Cancer Clinical Manifestations

image source: ahns.info
Most cancers do not produce any symptoms in early stages, the main sign is a palpable nodule in the thyroid. If the nodule is large enough to compress the trachea or esophagus, it can cause shortness of breath, difficulty swallowing, or "tingling" in the throat. Rarely, it can cause hoarseness if cancer irritates the laryngeal nerves found in the neck.
Thyroid Cancer Diagnosis
Blood tests are generally not helpful in diagnosing thyroid cancer, and thyroid tests such as TSH are usually normal, even when cancer is present. The examination of the neck by your doctor is the most common way the nodules are identified. The results of a fine-needle aspiration biopsy of a thyroid nodule allow the diagnosis of thyroid cancer to be established. While thyroid nodules are very common, less than 1 in 10 will turn out to be thyroid cancer.
Often, thyroid nodules are found incidentally in imaging tests such as CT scans and neck ultrasounds performed for reasons unrelated to the thyroid. Sometimes, the same patients can find the nodules by noticing a lump in the neck when looking in a mirror, by buttoning the shirt or putting on a necklace.
Have A Question About Thyroid Cancer Screening, Prevention or Treatment?
Contact Our Office.
Call 720.893.9515
Thyroid Cancer Treatment
Surgery
The primary treatment for all forms of thyroid cancer is surgery. The surgical procedure used will depend on the clinical conditions of the patients and the size of the tumor. In cases where there is an invasion of lymph nodes and the tumor spreads to the tissues surrounding the thyroid, performing a total thyroidectomy (complete removal of the thyroid) is the best option. In case of very small cancers (<1 cm) that are limited to the thyroid, affecting only one lobe and without evidence of having affected the lymph nodes, a simple lobectomy (exeresis of the lobe that has the tumor) is sufficient.
After surgery, most patients need to take thyroid hormone for life. Often, thyroid cancer is cured by surgery alone, especially if the tumor is small. If cancer inside the thyroid is large or if it has spread to the lymph nodes in the neck, or if your doctor thinks you have a high risk of recurrence, radioactive iodine may be used after the tumor is removed.
Radioactive Iodine Therapy

image source: cruk.org
Thyroid cells and most differentiated thyroid cancers absorb and concentrate iodine. That's why radioactive iodine can be used to remove residual cancerous tissue after surgery. This procedure is called ablation with radioactive iodine. Because most other tissues in the body do not absorb or concentrate iodine efficiently, the radioactive iodine used during the ablation procedure usually has little or no effect on other tissues. However, in some patients receiving higher doses of radioactive iodine for the treatment of thyroid cancer metastases, radioactive iodine can affect the glands that produce saliva and result in complications such as dry mouth. The use of high doses increases the risk of developing other cancers. The potential risks of treatment can be minimized by using the smallest dose possible.
Before starting treatment with radioactive iodine, it is necessary to increase the level of TSH in blood to favor the absorption of radioactive iodine, which can be achieved in two ways:
The first is to stop the thyroid hormone pills (levothyroxine) for 3-6 weeks. This results in the body producing high levels of TSH naturally. This will result in hypothyroidism, which can bring symptoms such as fatigue, cold intolerance, among others. To minimize the symptoms of hypothyroidism, your doctor may indicate T3 (liothyronine), a short-acting form of thyroid hormone, which is taken after stopping levothyroxine and up to two weeks before treatment with radioactive iodine.
Alternatively, TSH can be increased enough without stopping thyroid hormone, by parenteral administration of TSH. The benefit of this method is that you can continue treatment with thyroid hormone and avoid the possible symptoms related to hypothyroidism.
Regardless of the method used to raise TSH levels, the doctor should indicate a low iodine diet for 1 to 2 weeks before treatment which will result in improved radioactive iodine absorption, maximizing the effect of the treatment.
Advanced Thyroid Treatment
Distant metastasis of thyroid cancer is rare, but it can be a serious problem. Surgery and radioactive iodine are still the best way to treat these cancers. However, for more advanced cancers, or when radioactive iodine therapy is no longer effective, other forms of treatment will be needed. External radiation makes it possible to direct X-rays focused very precisely on the areas that must be treated, such as tumors that have reappeared after treatment with radioactive iodine or those that have spread to the bones or other organs. This can kill or slow the growth of those tumors.
New chemotherapeutic drugs have been used to treat metastatic thyroid cancer, including sorafenib and lenvatinib. These drugs rarely cure advanced cancers that have spread throughout the body, but they can slow or partially reverse tumor growth and extend patients' life expectancy. These treatments are usually administered by the oncologist and often require care at a medical center.
Clinical Follow-up
Regular follow-up exams are essential for all patients with thyroid cancer because this cancer can recur, even many years after successful treatment. The follow-up should include a complete medical history and a careful physical examination, with special attention to the neck area. Ultrasound of the neck is an important tool to visualize the neck and look for nodules, lumps or cancerous lymph nodes that could indicate that cancer has returned.
The majority of patients whose thyroid cancer has been removed require replacement of thyroid hormone with levothyroxine. The dose of levothyroxine recommended by your doctor will be determined in part by the initial extent of your thyroid cancer. More advanced cancers usually need higher doses to suppress TSH. In cases of cancers of minimal or very low risk, it is considered safe to keep the TSH in the normal range. The level of TSH is a good indicator of whether the dose of levothyroxine is adjusted correctly, and should be followed periodically by your doctor.
It consists of the application of high energy x-rays or radioactive particles to destroy cancer cells. It can be used as a single treatment before surgery or in combination with chemotherapy.
Explore Cancer & Disease Prevention, Screening, & Treatment
Have A Question About Thyroid Cancer Screening, Prevention or Treatment?
Contact Our Office.
Call 720.893.9515
Sources
1. Abu-Ghanem S, Cohen O, Lazutkin A, Abu-Ghanem Y, Fliss D,y Yehuda M. (2015). “Evaluation of clinical presentation and referral indications for ultrasound-guided fine-needle aspiration biopsy of the thyroid as posible predictors of thyroid cancer”. Head & neck. pag 1-5 DOI: 10.1002/ hed.24143.
2. Brito J, Davies L. (2014). “Is there an increased incidence of thyroid cancer?”. Current Opinion in Endocrinology, Diabetes and Obesity. 21(5): 405-408.
3. Clayman G. (2015). “Local Treatment of Differentiated Thyroid Carcinoma”. Clinical advances in Hematology & Oncology. 13(4):6-8.
4. Devita V, Lawrence T, Rosenberg S. “Devita, Hellman and Rosenberg´s Cancer Principles & Practice of Oncology”. 10th edition. Wolters Kluwer Health. USA .2015. pag 1175-1187.
5. O´Connell L, Prichard R, O´Reilly E, Skehan S, Gibbons D, McDermott E. (2015). “Runnig in the family: A rare diagnosis of familial papillary thyroid”. Elsevier, International Journal of Surgery Case Reports. 16: 64-66.
6. Wirth L. (2015). “Targeted Therapy for Advanced or Metastatic Differentiated Thyroid Carcinoma”. Clinical advances in Hematology & Oncology. 13(4): 9-16